| Description |
|
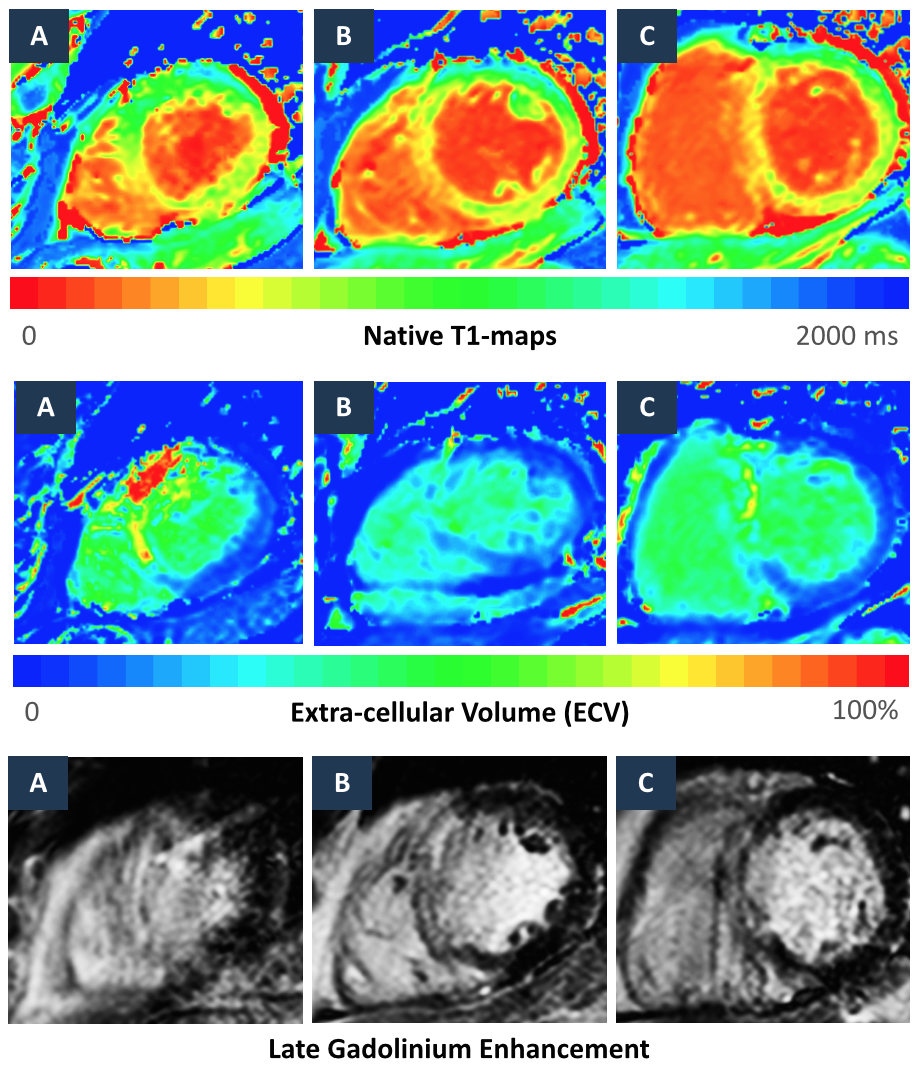 Apical (A), mid-ventricular (B) and basal (C) Native T1-maps, ECV-maps and corresponding LGE imaging for a patient with large septal infarct.
Apical (A), mid-ventricular (B) and basal (C) Native T1-maps, ECV-maps and corresponding LGE imaging for a patient with large septal infarct. |
| Tips and Tricks |
|
 |