| Protocol |
|
| Report |
|
| Key Points |
|
| Tips and Tricks |
|
| Aortic diameters |
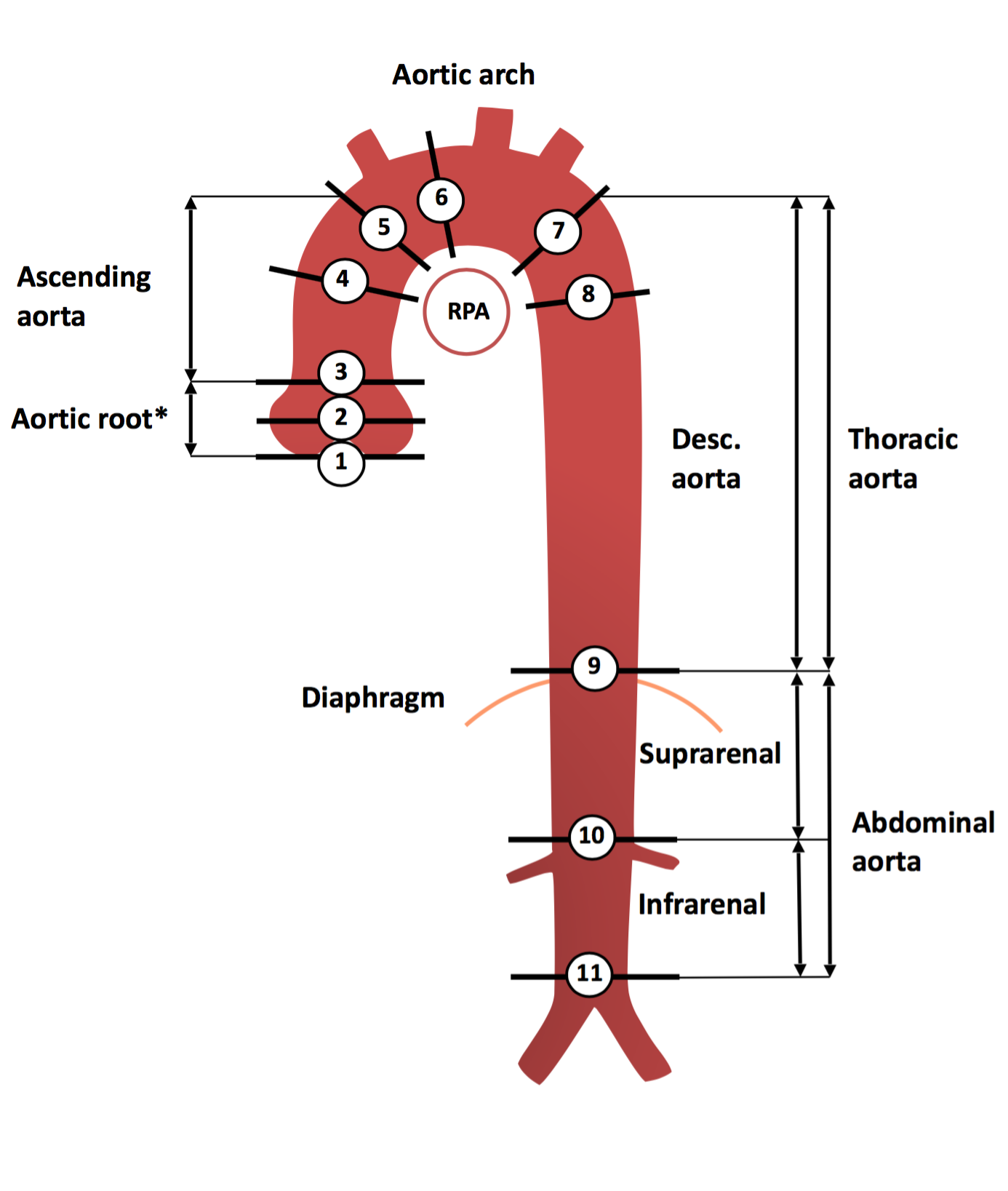 1. Aortic annulus,
2. Sinuses of Valsalva,
3. Sinotubular junction,
4. Mid ascending aorta (level of the pulmonary arteries),
5. Proximal aortic arch (at the origin of the brachiocephalic trunk),
6. Mid aortic arch (btw. left common carotid and subclavian arteries),
7. Proximal descending thoracic aorta,
8. Mid descending aorta (level of the pulmonary arteries),
9. At diaphragm,
10. At the celiac axis origin,
11. Immediately proximal to aortic bifurcation.
1. Aortic annulus,
2. Sinuses of Valsalva,
3. Sinotubular junction,
4. Mid ascending aorta (level of the pulmonary arteries),
5. Proximal aortic arch (at the origin of the brachiocephalic trunk),
6. Mid aortic arch (btw. left common carotid and subclavian arteries),
7. Proximal descending thoracic aorta,
8. Mid descending aorta (level of the pulmonary arteries),
9. At diaphragm,
10. At the celiac axis origin,
11. Immediately proximal to aortic bifurcation. |
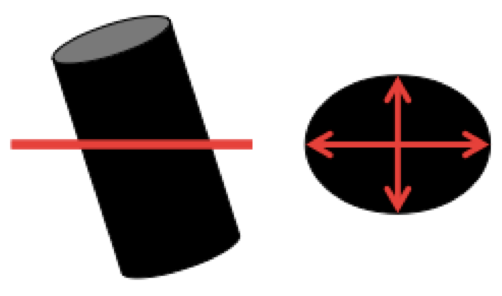
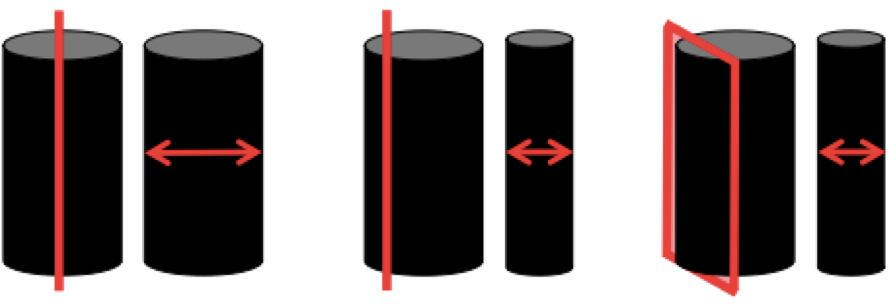
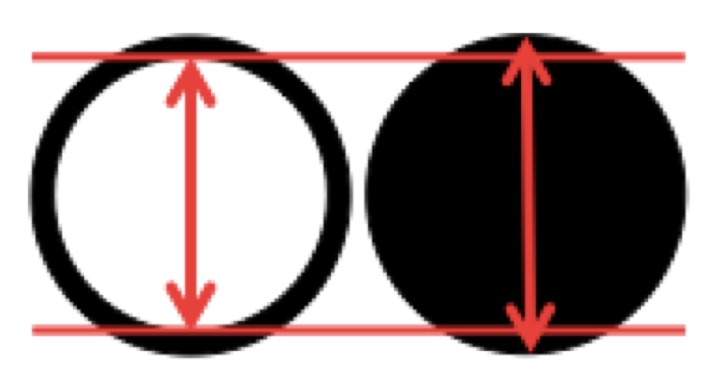
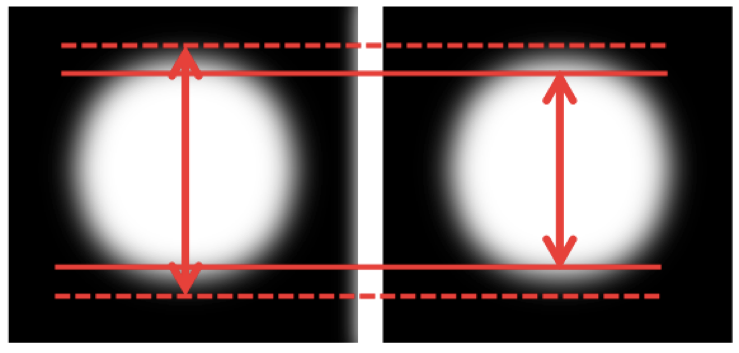
| Caveats of aortic measurements |
|
|
|
|
|
|
|
|
|
|
| References |
|